AsianScientist (Oct. 14, 2020) – Half a year into the worst pandemic in recent memory, a peculiar pattern is emerging: COVID-19 appears to be killing people in the rich, developed nations of the West at far higher rates than those in Asia. The pattern holds—for now—even in impoverished South Asian nations with densely-packed metropolitan areas and limited access to healthcare.
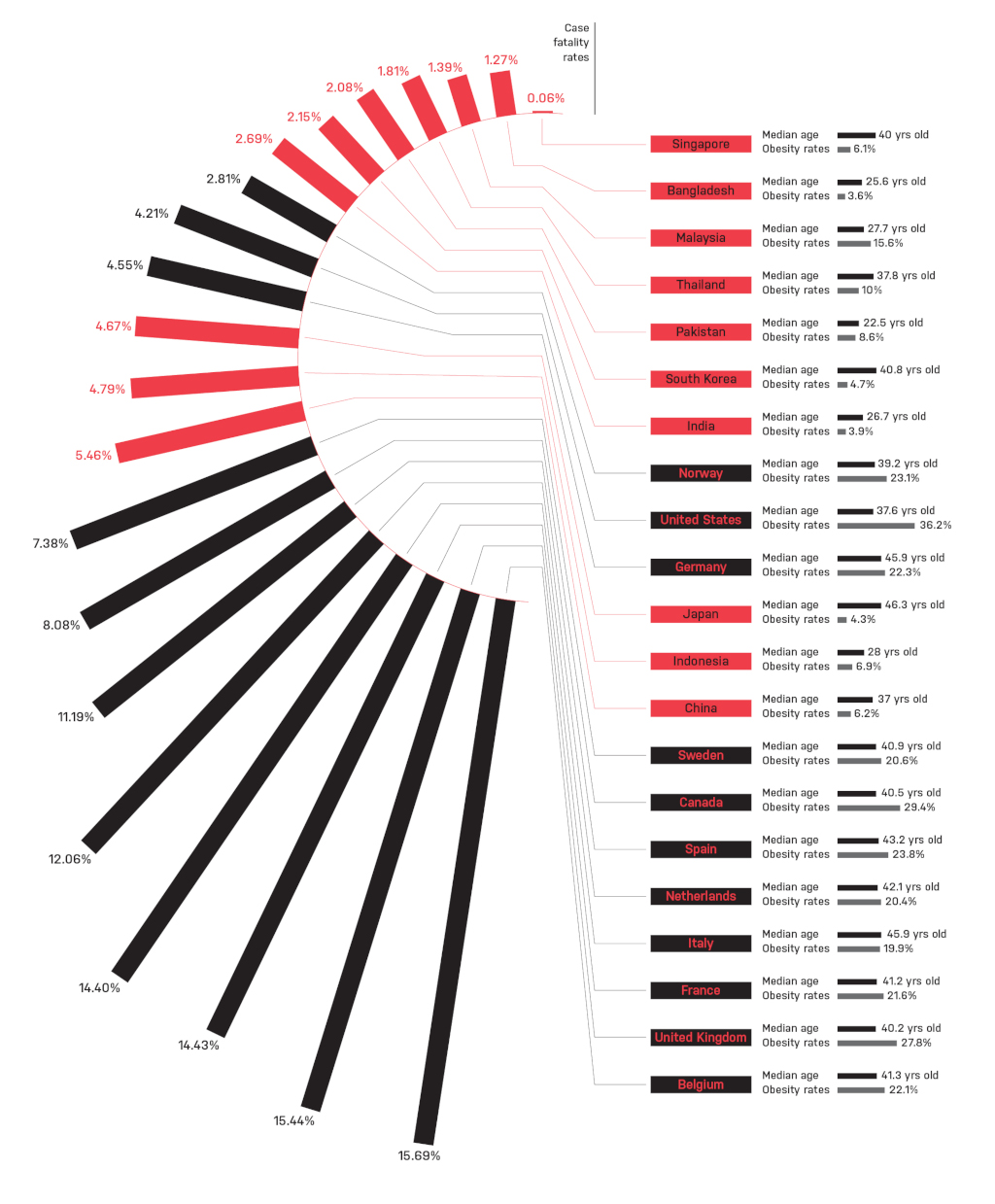
A quick glance at this chart built using data from John Hopkins University shows the striking trend. While COVID-19’s case fatality rate (CFR) in Europe is almost 12 percent, the CFR across Asia defies expectations at under three percent. It is also worth noting that the European CFR is more than double the global CFR of 4.5 percent.
The challenge of counting cases
On the one hand, experts caution that we should not make too much out of this unexpected finding. CFR—the number of deaths divided by the number of cases—is not a reliable indicator of a disease’s true impact while the pandemic is still ongoing. Instead, it is more of a snapshot of the best-available data at a single point in time during the pandemic.
“I would say that there is probably fairly poor quality of reporting across the world,” Dr. Jeremy Lim, an associate professor of global health at the National University of Singapore’s Saw Swee Hock School of Public Health, said.
Although it seems fairly straightforward to count the number of people who died due to COVID-19, in reality, there is considerable variability in reporting among countries. For instance, Belgium includes possible COVID-19 deaths in its count, those who died with COVID-like symptoms but were not tested for SARS-CoV-2.
On the flipside, looking at ‘excess mortality’—which compares the number of deaths at a given time with the historical average—suggests that some countries are undercounting their COVID-19 deaths. A comparison made by The Economist showed that the reported COVID-19 death toll in Italy in March and April made up only 64 percent of the country’s excess deaths, leaving over 14,000 ‘excess deaths’ unaccounted for. In contrast, Belgium’s COVID-19 deaths were more than 100 percent of its excess mortality, indicating a possible over-count.
In Asia, particularly the rural regions, COVID-19 deaths may be occurring outside of hospitals without ever being reported. Professor Dale Fisher, an infectious diseases consultant at Singapore’s National University Hospital, noted that reporting of deaths among some Asian countries may be unreliable—India, for example, added 2,003 cases on June 17 due to catch-up reporting. A pre-print study that analyzed Wuhan’s cremation services between February and March suggested some 36,000 deaths may have occurred, over ten times the 2,524 official deaths reported in the same period.
For all the difficulties in figuring out true COVID-19 death numbers, determining the number of infections is even harder.
“While the number of deaths resulting from COVID-19 is easier to account for—even then, there can be inaccuracies of reporting—the denominator, which tracks the number of infected patients, is much more variable,” Professor Quek Swee Chye, chairman of the medical board at National University Hospital in Singapore, shared with Asian Scientist Magazine.
Typically, the higher the testing rates, the lower the mortality, as a larger number of cases will dilute the number of deaths. However, at almost 1.5 million cases, the likelihood is small that Europe’s high CFRs were inflated due to under-testing. Even though the data is not clean, the difference in CFR between Europe and Asia is worth questioning.
“The magnitude of the difference is so large that we have to ask: are they real differences?” Lim said.
The elderly at risk
Age was very quickly identified as a big risk factor in COVID-19 severity and mortality. In early February, the Chinese Center for Disease Control and Prevention published data showing that those over 70 years old accounted for 50.8 percent of all COVID-19 deaths, even though they comprised only 12 percent of cases. For every extra decade of life, CFR rose steadily: 1.3 percent for those in their fifties, 3.6 percent for those in their sixties, 8.0 percent for those in their seventies and 14.8 percent for those in their eighties.
While Europe shows a more homogeneous pattern of an older population, Asia is more diverse in population age. Several nations like South Korea and Japan are comparable to European age, while Bangladesh, Malaysia, Pakistan, India and Indonesia are almost a decade younger. Although Singapore appears to be an anomaly as a country with a relatively high median age but low CFR, over 90 percent of COVID-19 infections in Singapore have occurred among younger migrant workers from South Asia.
There are also older populations that seem to have weathered COVID-19 fairly well, suggesting that age alone does not predict COVID-19 mortality. Japan and Germany, for instance, both have median ages over 45 like Italy, but have CFRs of 4.67 percent and 4.55 percent respectively, compared to Italy’s at 14.4 percent.
Obesity as co-morbidity
At least in the United States, obesity has been linked to higher severity COVID-19 outcomes. In fact, a study of 4,103 COVID-19 patients in New York City found that obesity was the second-strongest predictor for hospitalization risk after age. Those with a body mass index over 40 kg/m2 were almost twice as likely to develop critical illness.
Here, there is a clear pattern: obesity rates in Asian countries average below 10 percent, while Western nations average over 20 percent.
Taking the two risk factors of age and obesity together, Japan’s elderly population may have been spared the worst of COVID-19 by their low rates of obesity. Developing Asian nations with both young populations and low obesity rates like Bangladesh, Pakistan, India and Indonesia could also have benefited from their demographics.
The quality of care
Still, age and obesity aren’t sufficient to explain the whole picture: Germany, for instance, has a similar population density, aging population and obesity rates compared to neighboring France or Italy, yet has a much lower CFR.
“One of the major determinants of mortality is capacity to cope,” Quek said.
This includes infrastructural capacity like hospitals, intensive care units, ventilators and manpower capacity.
“There is a tipping point or threshold, beyond which even the best will be overwhelmed. This happens when there are big waves of patients.Once healthcare facilities and manpower are overwhelmed, the outcomes will be affected,” Quek added.
One indicator of capacity to cope is the number of intensive care unit (ICU) beds per capita. At the height of Europe’s COVID-19 pandemic, it is plausible that Germany staved off overwhelming of its healthcare system because of larger capacity: it has a whopping 29.2 ICU beds per 100,000 people, compared to an average of just ten among its neighbors. By late March, German hospitals started caring for COVID-19 patients from France and Italy as well.
A matter of time
As with past pandemics, only when the COVID-19 pandemic is over will its true mortality rate become clear. Looking at the number of COVID-19 deaths over time, trajectories for three South Asian countries—India, Bangladesh and Pakistan—are still rising while most in Europe have already peaked, Fisher noted.
Beyond the obvious risk factors of age and obesity for COVID-19 severity and the capacity of a healthcare system to help patients survive the disease, given the magnitude of difference in CFR, there may be other factors that warrant further study, Lim said. Those include regional variations in diet or whether innate differences in immunity to novel pathogens exist in different populations.
“We are living in an era of molecular genetics and a much deeper understanding of fundamental biology,” Lim said. “I would certainly make an appeal for more research.”
This article was first published in the July 2020 print version of Asian Scientist Magazine.
Click here to subscribe to Asian Scientist Magazine in print.
———
Copyright: Asian Scientist Magazine.
Disclaimer: This article does not necessarily reflect the views of AsianScientist or its staff.